

 Reply With Quote
Reply With Quote
Originally Posted by upthemaggies

Haha. That's brilliant. Nice one.

|
| + Visit Notts. County FC Mad for Latest News, Transfer Gossip, Fixtures and Match Results |
Results 431 to 440 of 568
-
17-12-2021, 12:23 PM #431
 Hall Of Fame
Hall Of Fame
- Join Date
- Jun 2003
- Posts
- 18,918
Nice unbiased re-title. Originally Posted by SwalePie
"Conspiracy theory" has lost its' potency however, it's effectively code for spoiler alert now with the Sage stats and government promises that "we won't be doing that" consistently proved wrong and the so called conspiracy theorists calling it right every step of the way.
-
17-12-2021, 12:27 PM #432
Hall Of Fame
- Join Date
- Aug 2006
- Posts
- 6,918
-
17-12-2021, 12:40 PM #433
Hall Of Fame
- Join Date
- Feb 2008
- Posts
- 6,553
Ok well that was a bit sneaky putting the quotation marks after 'on the latest government report' if it wasn't from the report. Originally Posted by upthemaggies
Anyway could you provide a link to whomever wrote that opinion so I can look at it in context?
As I said before the info in that report as a whole is quite useful to help judge some of the other claims made here, for example it says the immunity given by the vaccine is only slightly less effective after five months, whereas it has been claimed on here that it effectively only lasts ten weeks.
I also didn't see anything to back up the claims in the post of yours I've quoted, in fact if memory serves the government report shows vaccinated people are less likely to be infectious, less likely to be ill, to be hospitalised, and to die.
It also states that from tests carried out randomly on blood samples they think around 28% (again from memory) of the population has natural immunity, which when added to the around 70% who have vaccine induced immunity, would leave a small number who have neither natural immunity nor have been vaccinated, and it is intuitive, to me at least, to think they would be the ones needing proportionally more attention from the NHS, rather than the double jabbed filing up the hospitals, as you claim.
But I'd need to know which page the graph is from and look at it in context to be able to interpret it properly.
-
17-12-2021, 12:49 PM #434
Hall Of Fame
- Join Date
- Nov 2004
- Posts
- 24,769
Yes I thought it best to separate the conspiracy theory camp from the genuinely and honestly pro and anti vaccine camps. Glad you appreciate the lack of bias although personally I think your point in bold is rather far-fetched (but each to their own of course). Originally Posted by upthemaggies

Last edited by SwalePie; 17-12-2021 at 12:53 PM.
-
17-12-2021, 12:49 PM #435
Hall Of Fame
- Join Date
- Jun 2003
- Posts
- 18,918
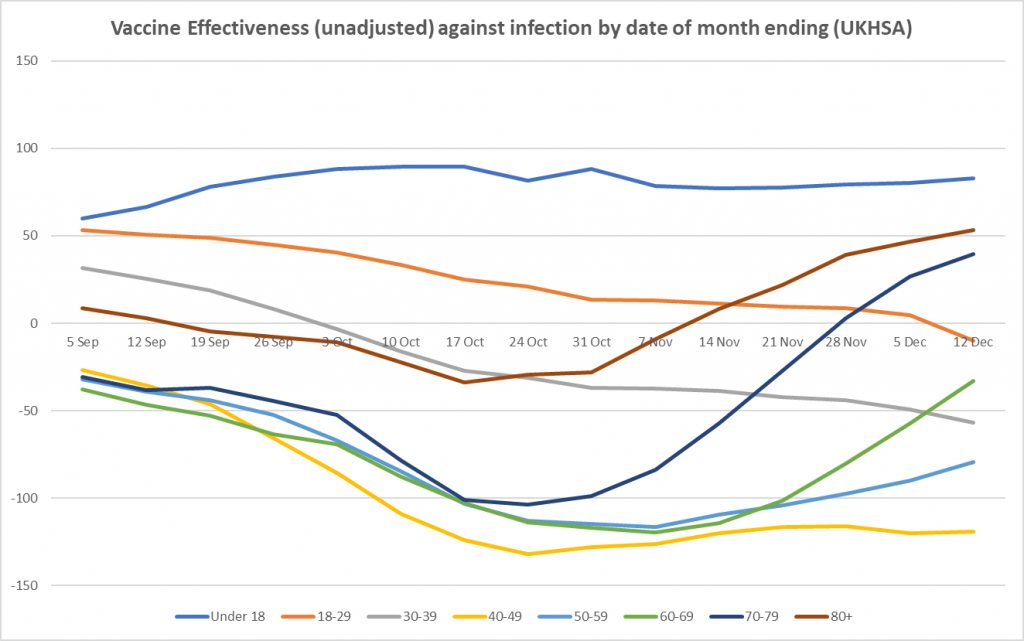
Vaccine Effectiveness Drops Below Zero in 18-29 Year-Olds for First Time – But Boosters Appear to be Helping Originally Posted by drillerpie
The latest UKHSA Vaccine Surveillance report, containing data for the month ending December 12th, brings mixed news on the vaccines. First the bad news. Unadjusted vaccine effectiveness based on the raw reported infection rates is still negative for all aged between 18 and 70 (see above). In fact, it’s gone negative for the first time in 18-29 year-olds, down to minus-10.1%, after a sharp drop in the last week. A negative vaccine effectiveness means the infection rate per 100,000 people is higher in the vaccinated than the unvaccinated. This means that vaccine passports and vaccine mandates will be ineffective at preventing transmission, and indeed it implies that the vaccinated are actually a higher transmission risk than the unvaccinated. Far from protecting the vaccinated from the unvaccinated, then, as much current policy seems intended to do, perhaps the unvaccinated should be wary of the company of the vaccinated. For those in their 40s in particular, unadjusted vaccine effectiveness is minus-119%, meaning the vaccinated are more than twice as likely to be carrying the virus than the unvaccinated.
The goods news, however, is that the boosters appear to be having a significant impact. Unadjusted vaccine effectiveness has been rising in the older age groups for some weeks, and is now solidly positive in the over-70s, albeit at a not-very-impressive 39.5% in 70-79 year-olds and 53.3% in the over-80s. That this rise is likely due to the third doses is indicated by the fact it has occurred in staggered fashion in each age group, apparently in line with when boosters were rolled out.
What appears to be the case to the casual eye has been put more rigorously to the test by Dr. Richard J. Booth, a retired civil servant with a Ph.D. in mathematical statistics. In a new piece published by the Daily Sceptic today, Dr. Booth undertakes statistical analysis to compare the booster rollout rates in each age group with the changes in the relative reported infection rates to see if there is any correlation over time. He explains:
"It occurred to me that since the third doses have been deployed at different rates in the different age groups, it might be possible to observe, and analyse, a ripple of decreasing infection rates from older to younger people over the last few weeks. So I developed a statistical model for infection rates, including a value dependent on the week (because the epidemic progresses at a rather unpredictable rate from week to week), and a week-dependent value proportional to the number of people who two or more weeks earlier had had the third dose compared with the number having had at least the first dose. I divided out the infection rate data by its value in the first week, to put the different age ranges on the same footing."
He concludes that what appeared to be the case is validated by his model, and the booster rollout correlates well with the changes in relative infection rates.
"I conclude that though three doses of vaccines may have been effective from the outset, statistical support for that proposition via these sources did not become apparent until week 44’s data was published, when nearly half of over 80’s had had boosters two or more weeks earlier, but has been sustained since then. Of course, ‘statistical support’ is not a cast-iron proof, as correlation is not causation and there might be ‘unknown unknowns’ at work. Nevertheless it is highly suggestive that the prior statistical work on Covid vaccines is vindicated here."
While not all readers will follow every detail in Dr. Booth’s thorough and technical article, it is well worth checking out.
https://dailysceptic.org/2021/12/17/...to-be-helping/
-
17-12-2021, 01:19 PM #436
Hall Of Fame
- Join Date
- Jun 2003
- Posts
- 18,918
Crikey, just seen this questioned posed, I'd never considered it before.....
"What would Thatcher have done in response to the pandemic?"
-
17-12-2021, 01:58 PM #437
Hall Of Fame
- Join Date
- Feb 2008
- Posts
- 6,553
Ok so the graph is theirs (Daily Sceptic's). That's why I couldn't find it on the government report. Originally Posted by upthemaggies
The data the Daily Sceptic have plotted are on the government report, along with a large and frankly unmissable caveat, which reads:
1 Comparing case rates among vaccinated and unvaccinated populations should not be used to estimate vaccine effectiveness against COVID-19 infection. Vaccine effectiveness has been formally estimated from a number of different sources and is summarised on pages 5 to 14 in this report.
The case rates in the vaccinated and unvaccinated populations are unadjusted crude rates that do not take into account underlying statistical biases in the data and there are likely to be systematic differences between these 2 population groups. For example:
• people who are fully vaccinated may be more health conscious and therefore more likely to get tested for COVID-19 and so more likely to be identified as a case (based on the data provided by the NHS Test and Trace)
• many of those who were at the head of the queue for vaccination are those at higher risk from COVID-19 due to their age, their occupation, their family circumstances or because of underlying health issues
• people who are fully vaccinated and people who are unvaccinated may behave differently, particularly with regard to social interactions and therefore may have differing levels of exposure to COVID-19
• people who have never been vaccinated are more likely to have caught COVID-19 in the weeks or months before the period of the cases covered in the report. This gives them some natural immunity to the virus for a few months which may have contributed to a lower case rate in the past few weeks
2 Case rates are calculated using NIMS - a database of named individuals from which the numerator and the denominator come from the same source and there is a record of each individuals vaccination status. Further information on the use of NIMS as the source of denominator data is presented on page 33 of this report and in the further resources below.
Unadjusted case rates among persons vaccinated have been formatted in grey to further emphasise the caution to be employed when interpreting these data.
So my first instinct is to think that to write an article based on those data, but where the whole premise goes completely against the statistical guidance provided alongside the data, making no reference to those caveats, is that it is an article I don't really want to trust.
I would also say that in light of those caveats, and without further supporting data, I personally don't think your claim stands up.
-
17-12-2021, 02:05 PM #438
Hall Of Fame
- Join Date
- Aug 2006
- Posts
- 6,918
I'm no longer listening to Whitty or the medical community. I'm going with this guy.
https://www.youtube.com/watch?v=uREpls3sTyU
-
17-12-2021, 02:09 PM #439
Hall Of Fame
- Join Date
- Feb 2008
- Posts
- 6,553
The UKHSA report says the following about vaccine induced protection from infection (from page 11):
Effectiveness against infection
Although individuals may not develop symptoms of COVID-19 after vaccination, it is possible
that they could still be infected with the virus and could transmit to others. Understanding how
effective vaccines are at preventing infection is therefore important to predict the likely impact of
the vaccination programme on the wider population. In order to estimate vaccine effectiveness
against infection, repeat asymptomatic testing of a defined cohort of individuals is required.
Studies have now reported on vaccine effectiveness against infection in healthcare workers,
care home residents and the general population (13, 14, 15, 16). With the delta variant, vaccine
effectiveness against infection has been estimated at around 65% with Vaxzevria and 80% with
Comirnaty (4).
Effectiveness against transmission
As described above, several studies have provided evidence that vaccines are effective at
preventing infection. Uninfected individuals cannot transmit; therefore, the vaccines are also
effective at preventing transmission. There may be additional benefit, beyond that due to
prevention of infection, if some of those individuals who become infected despite vaccination
are also at a reduced risk of transmitting (for example, because of reduced duration or level of
viral shedding). A household transmission study in England found that household contacts of
cases vaccinated with a single dose had approximately 35 to 50% reduced risk of becoming a
confirmed case of COVID-19. This study used routine testing data so would only include
household contacts that developed symptoms and went on to request a test via pillar 2. It
cannot exclude asymptomatic secondary cases or mildly symptomatic cases who chose not to
request a COVID-19 test (17). Data from Scotland has also shown that household contacts of
vaccinated healthcare workers are at reduced risk of becoming a case, which is in line with the
studies on infection (18). Both of these studies relate to a period when the Alpha variant
dominated. An analysis from the ONS Community Infection Survey found that contacts of
vaccinated index cases had around 65 to 80% reduced odds of testing positive with the Alpha
variant and 35 to 65% reduced odds of testing positive with the Delta variant compare to
contacts of unvaccinated index cases (19).
-
17-12-2021, 02:14 PM #440
Hall Of Fame
- Join Date
- Jun 2008
- Posts
- 3,879
😂😂😂 that’s awesome Originally Posted by Mapperleypie

Forum Info
Footymad Forums offer you the chance to interact and discuss all things football with fellow fans from around the world, and share your views on footballing issues from the latest, breaking transfer rumours to the state of the game at international level and everything in between.
Whether your team is battling it out for the Premier League title or struggling for League survival, there's a forum for you!
Gooners, Mackems, Tractor Boys - you're all welcome, please just remember to respect the opinions of others.
Click here for a full list of the hundreds of forums available to you
The forums are free to join, although you must play fair and abide by the rules explained here, otherwise your ability to post may be temporarily or permanently revoked.
So what are you waiting for? Register now and join the debate!
(these forums are not actively moderated, so if you wish to report any comment made by another member please report it.)
